Tricuspid Regurgitation
Overview of tricuspid regurgitation
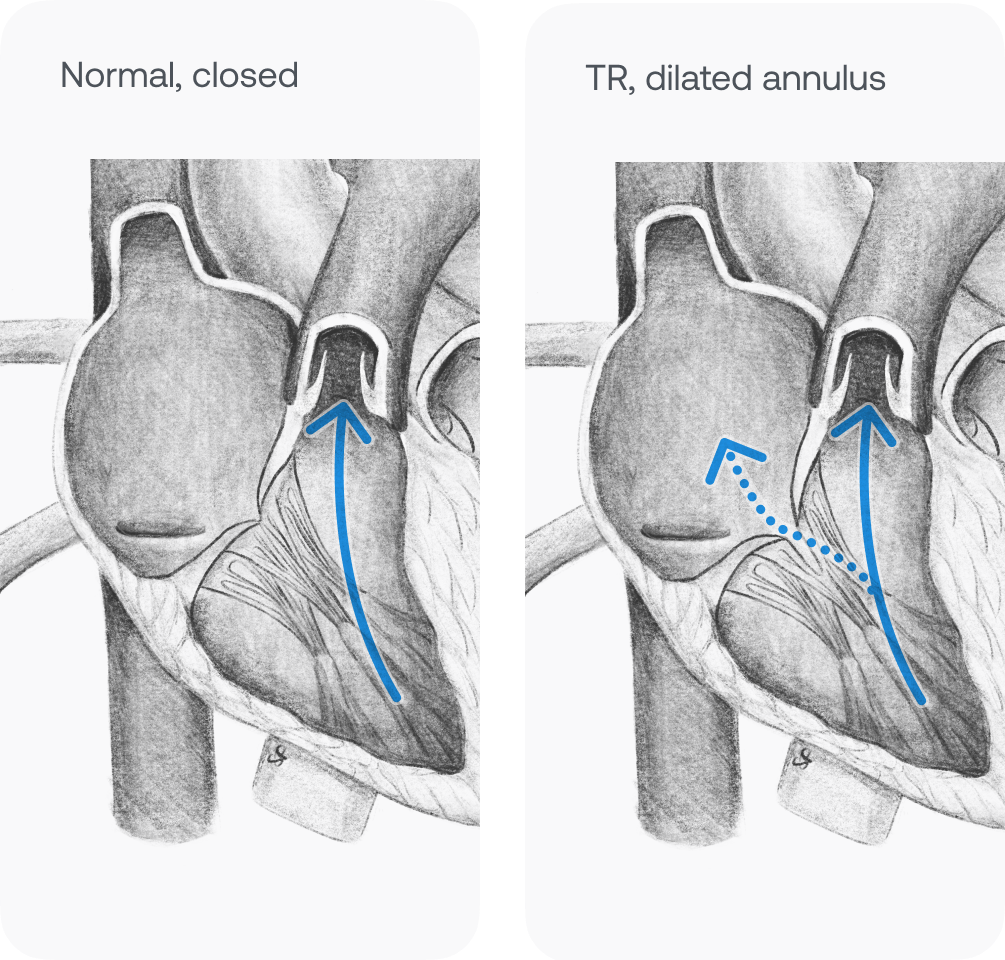
Tricuspid regurgitation (TR) occurs when the heart's tricuspid valve doesn't fully close, allowing blood to leak backward into the right atrium during systole. Trace/physiologic cases of TR aren't a cause for concern; they're common and present in 80% of otherwise healthy adults. Significant TR impacts 0.9% percent of the population. Untreated TR cases caused by valvular disease typically become more severe over time and lead to greater symptoms of right-sided heart failure. Mortality rates increase as TR worsens and some patients will require tricuspid valve surgery.1,2

Pathophysiology
Pathologic TR cases are caused by primary or secondary disruption of the normal function of the tricuspid valve. Approximately 10% of significant cases are primary; they're normally caused by rheumatic valve disease and congenital malformations like Epstein anomaly. The remaining 90% of cases are due to secondary causes including pulmonary hypertension, other valvular issues, or left-sided heart failure. Many of these conditions worsen over time if left untreated; right ventricle volume overload can lead to right-sided congestive heart failure, significant edema, and other symptoms like shortness of breath.2,3,4
Audio
Trace/physiologic TR is silent; TR progresses to a high-pitched, holosystolic, plateau murmur in moderate/severe cases. Pulmonary hypertension may cause S2 splitting and S3 or S4 may be present based on other heart pathology. This murmur is best heard at the lower left sternal border (fourth parasternal intercostal space location) while the patient is seated. The murmur becomes more pronounced when increasing venous return (leg raising, exercise) and inspiration (Rivero-Carvallo's sign). Standing and the Valsalva maneuver will make it decrease in severity.2,6

ECG
As seen below, there are normally no clear signs of TR on ECG. Other correlated ECG concerns are from secondary causes of TR: pulmonary hypertension, signs of MI, and atrial fibrillation. Pulmonary hypertension may cause right atrial hypertrophy which manifests on the lead II ECG as P pulmonale (P wave amplitude of > 2.5 mm).2,6,7

Actual recording
This sound was recorded using a stethoscope powered by Eko technology.
References
1. https://pubmed.ncbi.nlm.nih.gov/26358570
2. https://www.ncbi.nlm.nih.gov/books/NBK526121/
4. https://pubmed.ncbi.nlm.nih.gov/32921538/
5. https://www.thelancet.com/journals/lancet/article/PIIS0140-6736(16)00740-6/fulltext
6. https://www.ncbi.nlm.nih.gov/books/NBK345/
7. https://journals.sagepub.com/doi/full/10.1177/17534666221087846
Medical Advice Disclaimer
DISCLAIMER: THE CONTENT SET FORTH HEREIN DOES NOT PROVIDE MEDICAL ADVICE NOR IS AN ATTEMPT TO PRACTICE MEDICINE
The information, including but not limited to, text, graphics, images, and other material contained on this website are for informational purposes only. No material on this website or document are intended to be a substitute for professional medical education, advice, diagnosis, or treatment.
MKT-0002715 Rev 1.0
About the Author
