4 Standard Sounds Used to Evaluate Heart Health
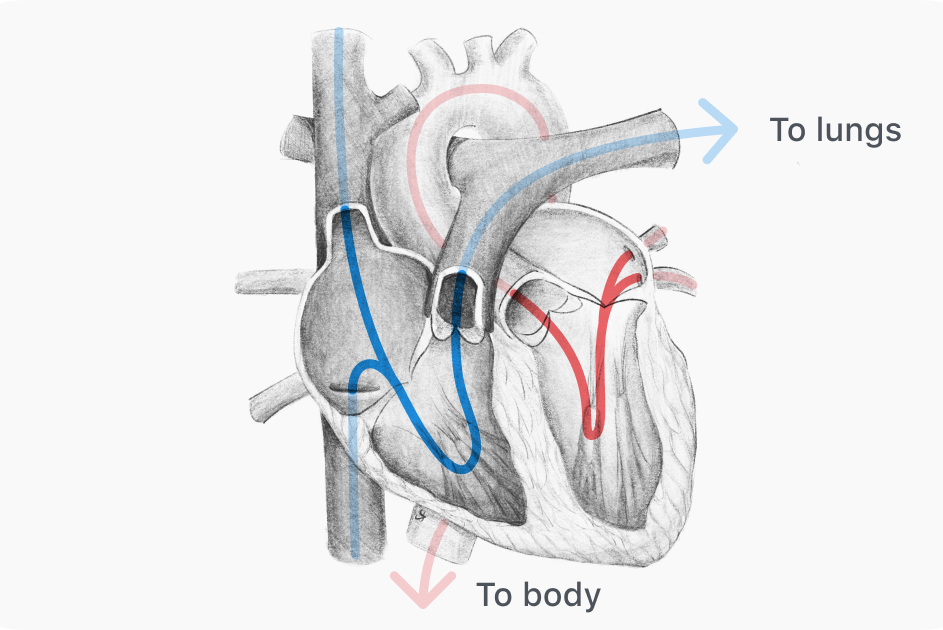
Overview of 4 standard heart sounds
One of the easiest tools to assess heart health is auscultation of heart sounds, both normal and pathologic. The familiar “lub” and “dub” are the two normal heart sounds, named S1 and S2, and are caused by the staggered closure of heart valves during the cardiac cycle. There are also two low-frequency heart sounds called S3 and S4, which are referred to as gallops and may or may not be present. An audible S3 can be normal or pathologic, while an audible S4 is always pathologic.
S1: Normal heart sound + ECG with S1, Q wave annotated

At the start of systole, the Q wave on an ECG marks when the ventricles become electrically activated and begin contracting. Shortly after this Q wave and contraction, the increasing ventricular pressure exceeds atrial pressure. Blood accumulates in the cusps of the atrioventricular (mitral and tricuspid) valves, forcing them closed to prevent backflow into the atria. The combined sound of these valves closing creates the first heart sound (S1), often recognized as the “lub” sound in the auscultation cycle. S1 is heard loudest at the cardiac apex, where it is normally louder than S2.
Sound recorded by Eko digital stethoscope technology:
S2: Normal heart sound + simplified PCG with S2 annotated

The second heart sound (S2) normally follows S1, comprising the "dub" sound marking the end of systole and beginning of diastole. S2 follows the T wave on an ECG, which represents ventricular repolarization. During systole, the semilunar valves (aortic and pulmonic) had been forced open to allow forward flow, but as the ventricles relax and depressurize, these valves close in sequence. These closures cause the sound known as S2, which is best heard at the base of the heart, auscultated at the right and left upper sternal borders. Aortic valve closure (A2) is heard best at the right upper sternal border, while pulmonic closure (S2) is loudest at the left upper sternal border.
Sound recorded by Eko digital stethoscope technology:
Split S2: Heart sound with split S2 with S1/A2/P2 annotated, ECG with T/Q annotated

During diastolic relaxation, the semilunar valves close when pressure above the valve exceeds pressure in the ventricle below. Aortic valve closure (A2) occurs slightly before pulmonic (P2) because of higher pressure in the aorta compared to the pulmonary artery. Together, A2 and P2 comprise S2, but when both sounds are heard distinctly this is called “splitting” of S2. Splitting varies throughout the respiratory cycle due to changes in intrathoracic pressure that affect blood flow. Normally, the duration between A2 and P2 increases during inspiration and decreases during expiration to become a single S2 sound. S2 splitting that does not vary with the respiratory cycle might indicate some underlying pathology.
Sound recorded by Eko digital stethoscope technology:
S3: Audio + ECG

When present, the abnormal third heart sound (S3) occurs in early diastole after S2. S3 is a low-frequency sound that results when an abnormally large volume of blood rapidly impacts the walls of the ventricle. This sudden deceleration of blood generates vibrations to create the S3 sound, best heard at the cardiac apex. S3 can be a normal finding in children, pregnant women, and athletes, but is generally abnormal in adults over 40. In this older population, a present S3 usually indicates ventricular overload or dysfunction, which could be due to heart failure, myocardial infarction, or other pathologies.
Sound recorded by Eko digital stethoscope technology:
S4: Audio + ECG

When present, the abnormal fourth heart sound (S4) occurs during late diastole just before S1, and is loudest at the cardiac apex. S4 is a low-frequency sound associated with rapid ventricular filling, which is a common characteristic of gallops — the category of extra heart sound that includes S3 and S4. While the exact mechanism is unknown, S4 is believed to be due to vibrations caused when blood flows in and strikes an abnormally stiff ventricular wall. Unlike S3, S4 is always pathologic when present and indicates a dysfunction of ventricular relaxation, most commonly due to heart failure.
Sound recorded by Eko digital stethoscope technology:
Medical Advice Disclaimer
DISCLAIMER: THE CONTENT SET FORTH HEREIN DOES NOT PROVIDE MEDICAL ADVICE NOR IS AN ATTEMPT TO PRACTICE MEDICINE
The information, including but not limited to, text, graphics, images, and other material contained on this website are for informational purposes only. No material on this website or document are intended to be a substitute for professional medical education, advice, diagnosis, or treatment.
About the Author
